The statements contained in this analysis are solely those of the authors and do not necessarily reflect the views or policies of CMS. The authors assume responsibility for the accuracy and completeness of the information contained in this document.
CMS’ announcement of the redesigned Global and Professional Direct Contracting (GPDC) program, now ACO REACH, created an opportunity for REACH participants to focus on health equity and to finally receive reimbursement payments that are adjusted to their patients’ specific needs. This post is the second part of a two-part series. Now that we understand how ACO REACH benchmarks and health equity adjustments are made, let’s focus on how to “Plan” and “Act” to implement health equity plans that tackle the main drivers of health equity.
CMMI has released preliminary guidance on the Health Equity Plan (HEP). The official PY2023 HEP will be due no later than March 31, 2023, which will be after REACH ACOs receive their PY2023 aligned beneficiary populations, to best identify and address disparities in their respective communities. CMMI has also created an opportunity to receive feedback on their proposed HEP in advance of the mandatory submission in March 2023. The optional preliminary HEP is due to CMS by September 16, 2022. More information on the preliminary submission can be found on CMS’ website.
A multidisciplinary workgroup is a great starting point for health equity intervention planning. Based on clinical quality frameworks pioneered by the Institute for Healthcare Improvement (IHI) as well as Lean methodology, this blog post will outline a process that can be considered best practice to establish and execute a health equity initiative at your organization.
Planning
The health equity planning process warrants the formation of a work group or committee, a governance structure for that committee, and a process to keep committee members accountable for not only planning but also executing on the health equity plan. Other key requirements for the committee:
- The committee should also be supported by executive leadership, including time and budgetary allowances necessary to execute a health equity plan for the organization. Ideally, the leader of the committee will report directly to a member of the C-suite or senior leadership.
- The committee should be multidisciplinary, with representation from departments within the organization that are involved in both caring for patients as well as leaders from operations, administration, and in some cases, community-focused departments. This blog post is written assuming that the broader organizational leadership has ’bought in’ to improving health inequity for their patients. Below is an example of the necessary committee members to compose and execute a health equity plan for an ambulatory primary care provider:
 | VP or Director, Population Health (‘Chair’ or committee leader) |
VP or Director, Administration and/or Operations | |
VP or Director, Nursing | |
VP or Director, Clinical & Quality Leader | |
VP or Director, Case Management | |
Data analysts, EHR experts | |
Project manager |






Accountability within the health equity planning committee is integral to ensuring that the plan is written and executed. Collaboratively establishing the committee’s goals, guiding principles, timeline, and specific roles and responsibilities during the kick-off allows input from the broader committee, creating a foundation for accountability among the team. Our favorite saying fits well here, ‘garbage in, garbage out.’ If the building blocks of forming the health equity plan are insufficient, then the health equity plan and its interventions will not help one’s patients and produce more equitable care.
Understanding The Drivers of Health Inequity in Your Patient Community
A health equity plan must be data-driven and tailored to the unique needs of one’s community. Though health equity plans across various organizations may look similar, each organization must ensure that their strategies to bridge health inequities are sensitive and specific to their population. ACO REACH requires not only the submission of a health equity plan but also performance under that plan by the ACO. To this end, data analysis of existing clinical and demographic data, and in some cases new data collection, must be the first step in the health equity planning process. Without measurable metrics as part of the health equity plan, the ACO will not be able to demonstrate improvements. Depending on the type of data that your organization has been collecting historically, it may also be helpful to work with local community-based organizations that can help identify drivers of health inequity (e.g., food insecurity, housing insecurity, access to care, access to pharmacy, etc.). The self-reported data required by the ACO REACH program is a good starting point.
The data analysts and EHR specialists on the committee will be crucial for this aspect of the planning process, as they are most familiar with the data. A literature review of peer-reviewed articles related to population health drivers, specifically studies that have similar populations to your patients, are also helpful guides to understand how to create analysis frameworks1,2. An organization may consider conducting a formal community needs assessment3, which many provider organizations publicly report periodically. The population health leader on the committee will determine if a formal community needs assessment is necessary, and further administrative and budgetary support from the broader organization may be required.
Identifying health inequities can be a daunting task as there are many factors that can be considered. Mutable vs. immutable factors is a distinction that is seen in many academic papers:
- ‘Immutable’ factors: race and dual eligible status (patients who are simultaneously eligible for Medicare and Medicaid)
- ‘Mutable’ factors: examples include food insecurity, lack of transportation, and other social determinants of health
For many organizations, however, data exploration will need to begin with the data that they have available to them. Most organizations have not yet collected sufficient data on the mutable factors to analyze their entire population.
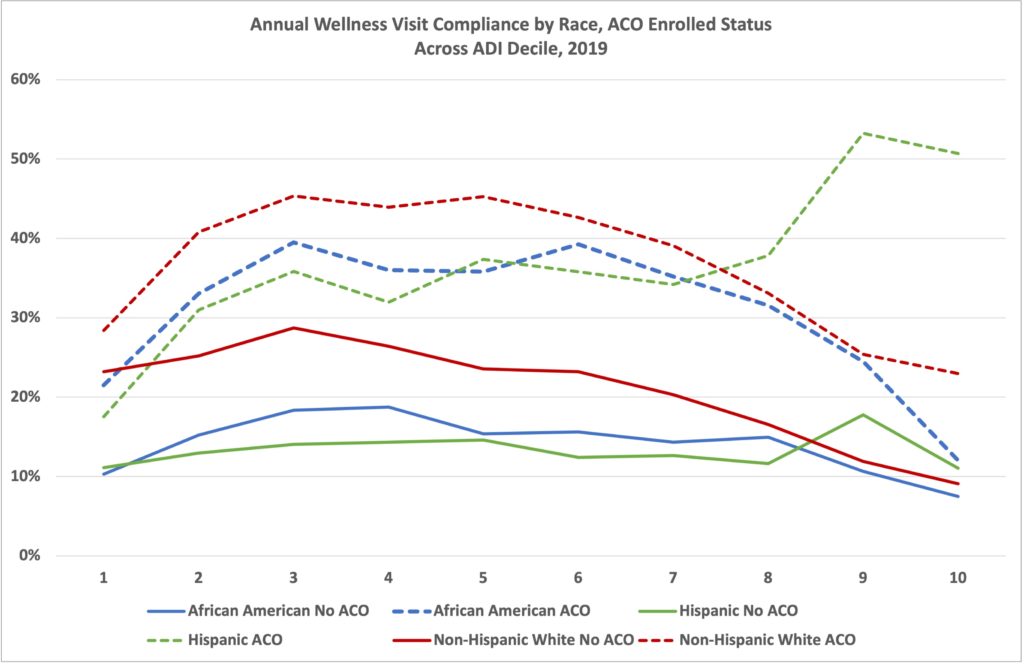
Most organizations are likely able to evaluate their populations along gender, race, age, geographic location, and Dual Eligibility axes. From these evaluations, organizations can dig deeper into why disparities exist within their organization and create action plans and goals around how to effectuate change. As an example, we looked at a simple preventive metric – Medicare Annual Wellness Visits (AWVs). This was broken down into:
- Race
- Dual-eligibility status
- Area Deprivation Index of the county in which the beneficiary resides
- Whether or not they are part of an Accountable Care Organization
- Note: We are only displaying African American, Hispanic, and White populations because each population represents over 10% of the population and the graphs get visually complex with additional data sets, but we are acutely aware of disparities also existing in the Asian/Pacific Islander population and especially the Alaskan-Native American populations