
Primary Care has long been considered the bedrock of a highly functioning healthcare system, where patients who enjoy trusted, longitudinal primary care relationships consistently experience better health, longer life expectancy, and lower overall healthcare costs. Unfortunately, in the United States alone, nearly 100 million adults lack access to primary care at a time when the primary care workforce faces a shortage of nearly 90,000 physicians over the next decade. Additionally, the United States is in the midst of a significant demographic shift where there are soon to be more Americans over the age of 65 than there are below 18. This aging population brings with it an epidemic of chronic diseases, obesity-related cardiometabolic-renal disease, cancer, neurocognitive diseases, and behavioral health concerns.
Extending high quality primary care to all Americans will require massive transformation of the prevailing care model and redesign of payment models to support it. Modern technology, specifically generative Al, now allows us to clearly envision a world where primary care is readily accessible to all – affordable, highly effective, proactive, personalized, and empathetic.
In this future vision, primary care transforms from a transactional series of office visits into a continuous ambient monitoring service where the “doctor’s office” is primarily a digital command center. In-person care becomes a high-precision logistical event, deployed only when physically necessary. “Going to the doctor” is replaced by “being with the doctor.” Al provides surveillance, novel financing provides incentives for prevention and innovation, and the human care team provides empathy and strategy.
Patient panels of 2,000 become 5,000 or greater. Valuable human capacity is used wisely. Patients get 24/7 access, convenience, and highly personalized care. Health outcomes improve and costs lower. This vision is no longer science fiction – this future is now.
The Agentic AI Unlock: Introducing Tom™
In early 2025, Lumeris introduced Tom, an Al operating system for primary care, and a new category of software – Primary Care as a Service (PCaaS). Built on over a decade of operating experience as a multi-population risk manager for millions of patients, working in partnership with many of America’s flagship health systems and large medical groups, Lumeris was an early adopter of generative Al using natural language to automate care processes.
The vision for Tom is to augment primary care physicians (PCPs) and their care teams by introducing the platform as an agentic Al “member of the care team” – charged with calculating for each patient in a primary care setting the “Best Next Action” to improve their health outcomes. Instead of handing a “gaps in care list” to a human, Tom autonomously takes the action – proactively outreaching for a cancer screening or vaccination, scheduling a post-hospital discharge follow-up visit, checking in on a patient with hypertension and diabetes to collect biometric data and ensure medication adherence, assessing symptoms, and hundreds of other clinically-relevant services common to primary care.
Tom also interacts with the primary care team – summarizing patient interactions and surfacing novel insights to the care team, providing “contextual” clinical decision support to providers at the point of care, and prioritizing patients that might need the practice’s attention. Strategic aggregators of primary care, namely health systems, quickly saw Tom as the tool that could finally allow them to imagine larger panels per PCP, drive better access, improve care model performance, declutter lower-acuity care from specialists while repatriating care back into primary care, and preserve continuity of downstream care within their own health systems.
Tom allows users to more clearly imagine the future of primary care.
Primary Care 2030: From Vision to Reality
The actor Robert Young’s portrayal of Marcus Welby, MD in the ABC television drama from 1969 to 1976 created the image for what became the cultural shorthand for the idealized, benevolent, all-knowing family doctor. Dr. Welby became the gold standard against which real-life primary care physicians were measured for decades. The nostalgia stems from a specific set of behaviors and a model of care that has become increasingly rare in modern medicine.
The image of Marcus Welby, MD persists as a powerful symbol of human connection in medicine. In an era of 15-minute appointment slots, electronic health records, and fragmented specialist care, Welby represents the desire to be known by one’s doctor, not just treated. Tom represents the modern technology-enabled opportunity to transform today’s sub-optimal experience of “going to the doctor” to “being with the doctor” – with many of the characteristics of a time that, until now, seemed forever lost in the past.
Features of “Nostalgic PCP”
Unrestricted Availability (The House Call)
A most enduring visual of Dr. Welby walking up a patient’s front path with black leather medical bag in hand, seemingly at any hour of the day or night.
The “Whole Person” Approach
Where the physical symptoms were treated within the context of the patient’s entire life cycle, and where Dr. Welby acted as doctor, therapist, social worker, and even father figure.
Holistic Care
Dr. Welby didn’t refer patients to specialists for every minor issue and managed most of the care himself.
Benevolent Paternalism
The character exuded a calm, authoritative demeanor, sat down and listened without looking at his watch (or computer screen), and offered reassurance that he would personally see the problem through to the end.
The Patient Experience: “Always-On” Care
Let’s envision the future with Tom. In the new model, the patient does not “go” to the doctor for a check-up, the doctor’s intelligence is constantly with them. The experience is characterized by frictionless access and pre-emptive intervention.
The Digital Front Door
The patient’s primary interface is a voice-enabled Al health assistant, Tom, via mobile phone or smart home device. This Al handles 80% of needs including care coordination, medication refills, appointment scheduling, and basic health coaching. Interactions are personalized to channel preferences (text vs. voice), language, and time of day.
Ambient Monitoring
Wearables and smart home sensors (smart mirrors, toilets, bedding, floor mats) continuously stream data. Tom analyzes trends in heart rate variability, sleep patterns, gait, or changes in the urine to predict illness before symptoms become acute.
The “Exception” Visit
When a physical exam is truly needed (for a biopsy, vaccination, or complex palpation), it does not happen in a generic crowded waiting room or medical clinic.
Instead, it can occur in a micro-clinic (500-sq-ft, high-tech neighborhood hub) or via a paramedicine-staffed mobile medical unit that comes to the patient’s driveway to avoid unnecessary ER trips for conditions like dehydration, CHF exacerbations, or minor infections.
The Role of AI: Tom as the “Infinite Resident”
Tom and its Al capability serves as the “cortex” of the practice, handling the cognitive load that currently contributes to physician burnout. It acts not just as a tool, but also as an always present, always “on” resident of sorts. Key responsibilities of Tom include:
Continuous Care Coordination & Risk Stratification
Algorithms audit the incoming stream of patient data 24/7. Tom “red flags” a patient whose weight gain and oxygen levels suggest early heart failure, escalating them to the top of a physician’s list explicitly before a crisis develops.
Automated Administrative Architecture
Tom summarizes patient interactions, proactively schedules appointments for specialty consultations, diagnostic tests, and ancillary services, refills medications, and interfaces with electronic health record-integrated tools (UM, ambient scribes, revenue cycle.)
Contextual Clinical Decision Support
In advance of an encounter, either asynchronous or synchronous (virtual or in-person), Tom prompts the human provider with “Best Clinical Guidance” based on what is known about the patient from a complete patient record and contemporaneous patient-derived insights, guiding care that is based on the latest global research. Not only does this act as a real-time safety net against error, it allows for “top of license” performance by each clinician on the care team.
The Role of the Primary Care Provider, Enabled and Augmented by Tom
With Tom handling data gathering and routine synthesis, human roles shift toward high-level strategy, empathy, trust, and complex patients and procedures. In this new world, the PCP manages a much larger panel of patients (potentially 5,000+ instead of 2,000) but only interacts with the top 5% of higher-risk or most complex cases. Their job is no longer data entry; it is synthesizing complex information and making high-stakes judgment calls.
The workspace is very different, more akin to a modern tech-forward command center. The PCP is continuously fed asynchronous tasks which Tom has teed up for rapid review and sign off with dynamic prioritization raising the more pressing items to the top. As the regulatory environment and scope of practice laws evolve, Tom will assume more autonomous action. Inside of these encounters, Tom summarizes patient interactions, displays any patient-generated data, provides clinical decision support prompts where able, and stands ready to execute any new orders from the physician.
Patients requiring the physician’s time are coordinated as well with telemedicine being the likely patient communication channel, with or without human facilitation at the patient’s side. The physician coordinates logistics with a practice coordinator to dispatch a mobile unit to the home or route a patient to a micro clinic site that is convenient, if palpation, physical examination, or diagnostics are likely required for accurate and efficient diagnosis.
Optimal Financing Model: “Subscription + Outcomes”
The traditional fee-for-service (FFS) model is incompatible with this vision because it incentivizes volume (in-person, E/M-billable clinical encounters) rather than value (healthier patients). The optimal payment model is a hybrid direct primary care (DPC) and capitation structure.

There are several ways that the subscription model could now come to life. Because Tom-enabled primary care can be provided at a predictable and affordable cost, insurance products can universally include it as a benefit, and employers or self-pay consumers can fund primary care through HSA/FSA benefits or other tax-incentivized policies – combined with catastrophic “wrapper” insurance coverage.
Alternatively, traditional carriers could contract fully insured lives using a PMPM payment model (in lieu of FFS for a defined set of services), even within PPO networks, using regular, Tom-facilitated, patient-defined attribution in lieu of claims-driven logic (where Tom confirms with patients quarterly that their PCP is still Dr. Smith.”)
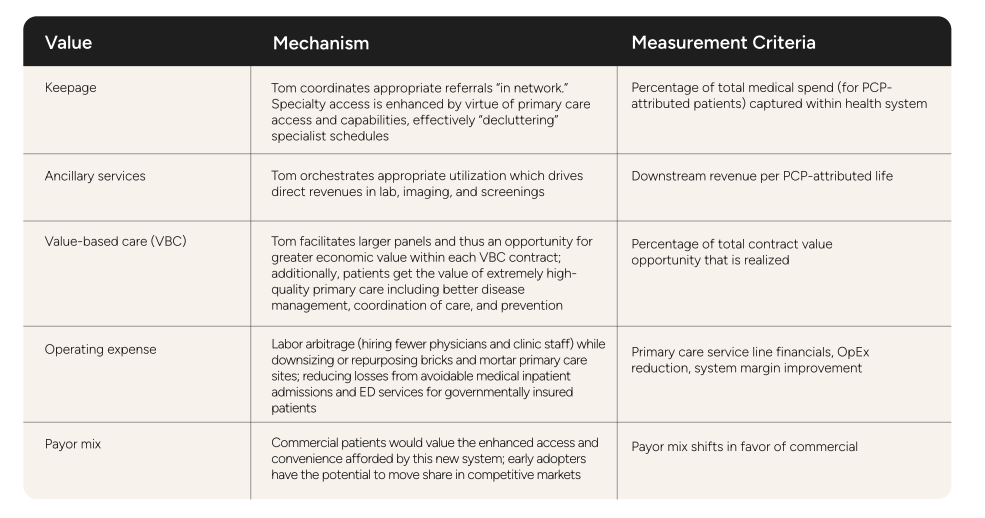
Health systems have additional ways to monetize more effective and efficient primary care with larger patient panels per PCP.
In Summary: The Future Is Now
Delivering high quality primary care to all Americans is now within our reach, thanks to the significant advances in generative Al. As with most transformations, technology itself is an important piece, but technology will fail to achieve its full potential in the absence of its adoption and deployment by humans. The art of the possible is only limited by our imagination and our willingness to evolve. Patients, healthcare providers, and purchasers all stand to gain by this new vision for primary care – but patients, rightfully, have the most to gain. Consider these three patients and how a Tom-enabled primary care practice would benefit them:
Health-Conscious Executive
For a patient focused on wellness and prevention, Al acts as a proactive coach, synthesizing data from their wearables to help optimize their routine and provide personalized insights. Care is remote and convenient allowing him to balance and protect his work and personal schedules.
Elderly Patient with Chronic Conditions
For an elderly patient with complex needs, Al provides a lifeline of continuous monitoring and support, connecting them to their care team and ensuring their conditions are managed effectively and proactively – mostly from the comfort of their own home.
Single Mother with a Behavioral Health Diagnosis
For a busy parent, Al offers accessible, on-demand mental health support, allowing them to check in with their care team and access resources discreetly and conveniently. The patient doesn’t have to sacrifice work or family for health.
Ai-Enabled Primary Care is a Reality
With Tom, Al enabled primary care is now a reality. Leading health systems across the country are embracing this incredible technology to solve one of the most vexing challenges in American health care – access to primary care, and all the benefits which accrue from that access. The future of primary care is indeed now.
Schedule a Tom Demo
References
Bhuyan, S. S., Sateesh, V., Mukul, N., Galvankar, A., Mahmood, A., Nauman, M., … & Samuel, J. (2025). Generative artificial intelligence use in healthcare: Opportunities for clinical excellence and administrative efficiency. Journal of Medical Systems, 49(1). https://doi.org/10.1007/s10916-024-02136-1
Daniel, H., Bornstein, S. S., & Kane, G. C. (2018). Addressing social determinants to improve patient care and promote health equity: An American College of Physicians position paper. Annals of Internal Medicine, 168(8), 577–578. https://doi.org/10.7326/m17-2441
Holman, H. R. (2020). The relation of the chronic disease epidemic to the health care crisis. ACR Open Rheumatology, 2(3), 167–173. https://doi.org/10.1002/acr2.11114
Jabbarpour, Y., Jetty, A., Byun, H., & Siddiqi, A. (2025). The cost of neglect: How chronic underinvestment in primary care is failing US patients. The health of US primary care: 2025 scorecard report. Milbank Memorial Fund. https://www.milbank.org/publications/the-health-of-us-primary-care-2025-scorecard-report/
Jones, C. H., & Dolsten, M. (2024). Healthcare on the brink: Navigating the challenges of an aging society in the United States. npj Aging, 10(1). https://doi.org/10.1038/s41514-024-00148-2
Lim, S. M., Li, P., Braat, S., Aung, Y. H., Fu, S., Johnson, D. F., & Lim, W. K. (2025). Validation of a multi-channel ambient sensor to measure vital signs in patients within the ward and at home. Sensors, 25(4), 1149. https://doi.org/10.3390/s25041149
McCarthy, M. (2015). Report predicts US physician shortage could exceed 90,000 by 2025. BMJ, 350, h1296. https://doi.org/10.1136/bmj.h1296
Milbank Memorial Fund. (2025). Building bridges to value: Infrastructure essentials for community health centers. https://www.milbank.org/publications/building-bridges-to-value/
Physician-Focused Payment Model Technical Advisory Committee (PTAC). (2025). Reducing barriers to participation in value-based care models. U.S. Department of Health and Human Services. https://aspe.hhs.gov/ptac-meetings
Starfield, B., Shi, L., & Macinko, J. (2005). Contribution of primary care to health systems and health. The Milbank Quarterly, 83(3), 457–502. https://doi.org/10.1111/j.1468-0009.2005.00409.x
Sun, X., & Li, X. (2023). Editorial: Aging and chronic disease: Public health challenge and education reform. Frontiers in Public Health, 11. https://doi.org/10.3389/fpubh.2023.1175898
Taylor & Francis. (2025). AI in primary care — a general practitioner’s bucket list. European Journal of General Practice, 31(1). https://doi.org/10.1080/13814788.2025.2567462